





|
A pioneer in its field, Echosens significantly changed the practice of liver diagnosis with FibroScan®, the non-invasive gold standard solution for comprehensive management of liver health. FibroScan® is recognized worldwide as the reference for liver fibrosis and liver steatosis assessment with more than 3,000+ peer-reviewed publications and 140+ international guidelines. Echosens has made FibroScan® available in over 100+ countries enabling millions of liver examinations worldwide. |
 |
 |
 |
 |
|
Products |
Liver Health |
User testimonials |
Information for patients |
| READ MORE | READ MORE | READ MORE | READ MORE |
FibroScan® Products
When evidence matters and consistency counts
- Pioneer in the field of liver elastography
- FibroScan® produces biomarkers that can assess and monitor patients over time
- FibroScan® uses uniform algorithms that minimize inter-operator variability and eliminate inter-system variability
- 6,500+FibroScan® installed worldwide enabling millions of liver examinations
- Winner of the Red Dot Design Award (FibroScan® Mini+ 430 model)
Which FibroScan® is right for you?
 |
Capabilities
Features
Ergonomics
|
 |
Capabilities
Features
Ergonomics
|
 |
Capabilities
Features
Ergonomics
|
Liver Health
Liver health has remained an unmet medical need on the global scale. People are not familiar with the liver. Despite the fact that it’s a vital organ, they may not know that liver health is critical. Chronic liver disease is increasing dramatically, but it can be reversible if diagnosed early and correctly monitored and treated.
The liver ID
The liver is a vital organ, situated on the right side, midway between the waist and the armpit. It is the largest organ of the body (length: 10 cm, weight: 1.4 – 1.6 kg) and one of the hardest working.
The liver is the toxin filter and vitamin reservoir of the body with 3 main functions: detoxify – synthesis – storage.
Chronic liver disease has become a major global health issue⁵
With an estimated worldwide prevalence of 2.5%, chronic liver disease is an increasingly major cause of morbidity and mortality.6
2 million deaths per year worldwide are caused by chronic liver disease.6,7
There are 3 main causes of chronic liver disease
A poor diet and a sedentary lifestyleNAFLD NASH |
 |
 |
Hazardous alcohol consumptionAlcoholic liver disease is responsible for 3 million deaths every year.*11 Globally, over 50% of cirrhosis-related mortality is attributable to alcohol. |
Viral infectionHepatitis C Virus Hepatitis B Virus |
 |
Silent and under-diagnosed
8 to 9 out of 10 people are unaware of living with viral hepatitis.*14
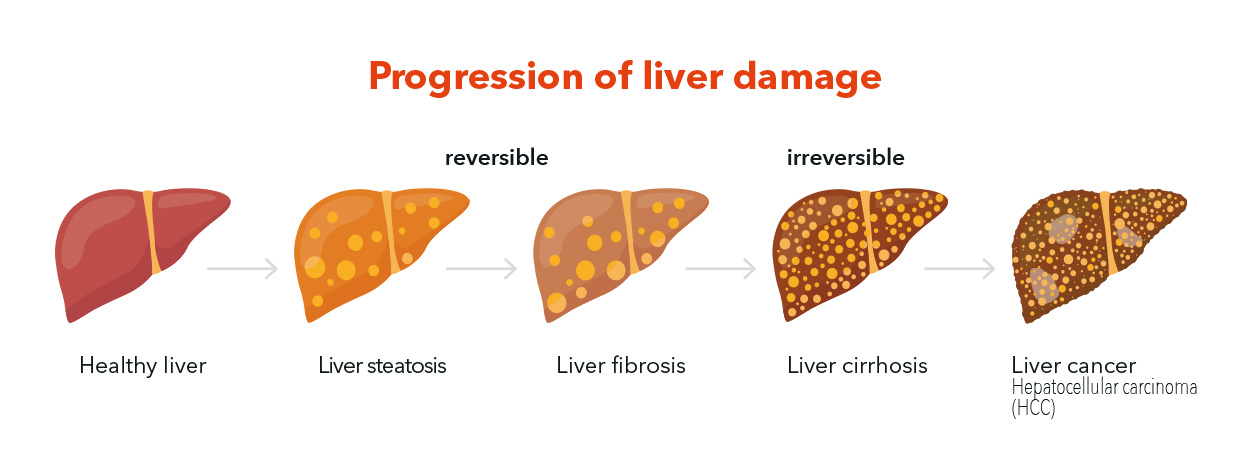
Mostly asymptomatic, chronic liver disease like NAFLD and NASH are silent but can potentially progress to cirrhosis or liver cancer (HCC).8,15
Cirrhosis is the end-stage of chronic liver disease. It is usually irreversible, with a poor prognosis once clinical decompensation has occurred. The only curative treatment option for decompensated cirrhosis is liver transplant.16
Damage to the liver caused by chronic liver diseases can often be reversed by early diagnosis and intervention.6
Our liver health solutions, FibroScan® and Scores by echosens allow a comprehensive management of liver health.
User testimonials
FibroScan® tried and trusted by healthcare providers
Our solutions support medical professionals across the world from different medical specialties. Discover why they chose FibroScan® for their clinical practice

As a clinical researcher, I rely heavily on FibroScan® to select the right patient for the right study. Clinical trials in non-alcoholic steatohepatitis typically include patients with specific fibrosis stages. It is thus important to have reliable fibrosis assessment and avoid unnecessary liver biopsies. |
|
While performing clinical research in the field of metabolic steatohepatitis, I am constantly asked how I can keep my screening failure rate low. The answer is no secret: FibroScan® examination with SmartExam. |
|
Assessment of liver stiffness and fat by non-invasive method is a huge step forward towards better management of NAFLD. It has hugely impacted the way clinicians stratify the patients, chose therapy and monitor response! |
|
There is very good evidence for using transient elastography by FibroScan® for assessment of fibrosis in alcohol-related liver disease. |
|
Using FibroScan® as an interventional therapy helps primary care physicians and nurse specialists engage patients by demonstrating the results and outcomes as a value change that patients can visualize on a regular basis and give them confidence that their efforts have an impact. […]Weight loss and exercise are the first step in mitigating liver damage. |
|
FibroScan® is perfect for use in a primary care setting, it is portable and gives patients an instant result enabling them to leave knowing the result. It is also a very powerful tool to encourage lifestyle interventions. Using the FibroScan® in primary care enables much wider access to this technology for patients and significantly reduces the cost per scan. |
Information for patients
Everything you need to know about your liver examination with FibroScan®.
FibroScan® is the gold standard non-invasive solution for comprehensive management of liver health. It is called non-invasive as nothing enters your body.
FibroScan® sends a pulse of energy to your liver, which will give your doctor important information about your liver’s health.
Watch our patient video
Reference
- European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237-264. doi:10.1016/j.jhep.2015.04.006.
- Karlas T, Petroff D, Sasso M, et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J Hepatol. 2017;66(5):1022-1030. doi:10.1016/j.jhep.2016.12.022.
- Recio E, Cifuentes C, Macías J, et al. Interobserver concordance in controlled attenuation parameter measurement, a novel tool or the assessment of hepatic steatosis on the basis of transient elastography. Eur J Gastroenterol Hepatol. 2013;25(8):905-911.doi:10.1097/MEG.0b013e32835f4c3d.
- Stefanescu H, Marasco G, Calès P, et al. A novel spleen-dedicated stiffness measurement by FibroScan® improves the screening of high-risk oesophageal varices. Liver Int. 2020;40(1):175-185. doi:10.1111/liv.14228.
- Ginès P, Graupera I, Lammert F, et al. Screening for liver fibrosis in the general population: a call for action. The Lancet Gastroenterology & Hepatology. 2016;1(3):256-260. doi:10.1016/S2468-1253(16)30081-4.
- Marcellin P, Kutala BK. Liver diseases: A major, neglected global public health problem requiring urgent actions and large-scale screening. Liver Int. 2018;38 Suppl 1:2-6. doi:10.1111/liv.13682.
- Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver diseases in the world. J Hepatol. 2019;70(1):151-171. doi:10.1016/j.jhep.2018.09.014.
- Wong VW-S, Adams LA, de Lédinghen V, Wong GL-H, Sookoian S. Noninvasive biomarkers in NAFLD and NASH – current progress and future promise. Nat Rev Gastroenterol Hepatol. 2018;15(8):461-478. doi:10.1038/s41575-018-0014-9.
- Kwok R, Choi KC, Wong GL-H, et al. Screening diabetic patients for non-alcoholic fatty liver disease with controlled attenuation parameter and liver stiffness measurements: a prospective cohort study. Gut. 2016;65(8):1359-1368. doi:10.1136/gutjnl-2015-309265.
- Younossi ZM. The epidemiology of nonalcoholic steatohepatitis. Clin Liver Dis (Hoboken). 2018;11(4):92-94. doi:10.1002/cld.710.
- Seitz HK, Bataller R, Cortez-Pinto H, et al. Alcoholic liver disease. Nat Rev Dis Primers. 2018;4(1):16. doi:10.1038/s41572-018-0014-7.
- WHO. Guidelines for the Screening Care and Treatment of Persons with Hepatitis C Infection. April 2014. http://public.ebookcentral.proquest.com/choice/publicfullrecord.aspx?p=1975017. Accessed March 4, 2020.
- WHO. Hepatitis B. https://www.who.int/news-room/fact-sheets/detail/hepatitis-b. Accessed February 14, 2020.
- WHO. Department of HIV/AIDS, the Global Hepatitis Programme. World Hepatitis Day 2017, WHO guide on advocacy and communications. 2017. https://www.who.int/campaigns/hepatitis-day/2017/campaign-brief.pdf?ua=1
- Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11-20. doi:10.1038/nrgastro.2017.109.
- Ahmad J, Lau. Clinical applications of the Model for End-Stage Liver Disease (MELD) in hepatic medicine. HMER. Published online February 2013:1. doi:10.2147/HMER.S9049.
- Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease: Estes et al. Hepatology. 2018;67(1):123-133. doi:10.1002/hep.29466.
- Ofusu 2018
- Friedman, 2018
- Lanthier, 2018
- Singal AK, Bataller R, Ahn J, Kamath PS, Shah VH. ACG Clinical Guideline: Alcoholic Liver Disease. Am J Gastroenterol. 2018 Feb;113(2):175-194. doi: 10.1038/ajg.2017.469 . Epub 2018 Jan 16. PMID: 29336434 ; PMCID: PMC6524956.
- Rehm, J. et al. Alcohol as a risk factor for liver cirrhosis: a systematic review and meta- analysis. Drug Alcohol Rev.29, 437–445 (2010).
- WHO. Hepatitis B. https://www.who.int/news-room/fact-sheets/detail/hepatitis-b. Accessed February 14, 2020.
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017 Aug;67(2):370-398. doi: 10.1016/j.jhep.2017.03.021. Epub 2017 Apr 18. PMID: 28427875.
- Lim JK, Flamm SL, Singh S, Falck-Ytter YT; Clinical Guidelines Committee of the American Gastroenterological Association. American Gastroenterological Association Institute Guideline on the Role of Elastography in the Evaluation of Liver Fibrosis. Gastroenterology. 2017 May;152(6):1536-1543. doi: 10.1053/j.gastro.2017.03.017. PMID: 28442119.
- Mederacke I, Wursthorn K, Kirschner J, Rifai K, Manns MP, Wedemeyer H, Bahr MJ. Food intake increases liver stiffness in patients with chronic or resolved hepatitis C virus infection. Liver International 2009;29:1500-1506.
- Arena U, Lupsor Platon M, Stasi C, Moscarella S, Assarat A, Bedogni G, Piazzolla V, et al. Liver stiffness is influenced by a standardized meal in patients with chronic hepatitis C virus at different stages of fibrotic evolution. Hepatology 2013;58:65-72.
- Berzigotti A, De Gottardi A, Vukotic R, Siramolpiwat S, Abraldes JG, Garcia-Pagan JC, Bosch J. Effect of meal ingestion on liver stiffness in patients with cirrhosis and portal hypertension. PLoS One 2013;8:e58742.
- Boursier J, Zarski JP, de Ledinghen V, Rousselet MC, Sturm N, Lebail B, Fouchard-Hubert I, et al. Determination of reliability criteria for liver stiffness evaluation by transient elastography. Hepatology 2013;57:1182-1191.
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67(1):328-357. doi:10.1002/hep.29367.
- Ferraioli G, Wong VW-S, Castera L, et al. Liver Ultrasound Elastography: An Update to the World Federation for Ultrasound in Medicine and Biology Guidelines and Recommendations. Ultrasound Med Biol. 2018;44(12):2419-2440. doi:10.1016/j.ultrasmedbio.2018.07.008.
- Shiha G, Ibrahim A, Helmy A, et al. Asian-Pacific Association for the Study of the Liver (APASL) consensus guidelines on invasive and non-invasive assessment of hepatic fibrosis: a 2016 update. Hepatol Int. 2017;11(1):1-30. doi:10.1007/s12072-016-9760-3.
- Audière et al. EASL 2020 poster #FRI-073.
- Cohen JC, et al. Science. 2011;332(6037): 1519- 1523.